EM 2023 Day Thank you for your support
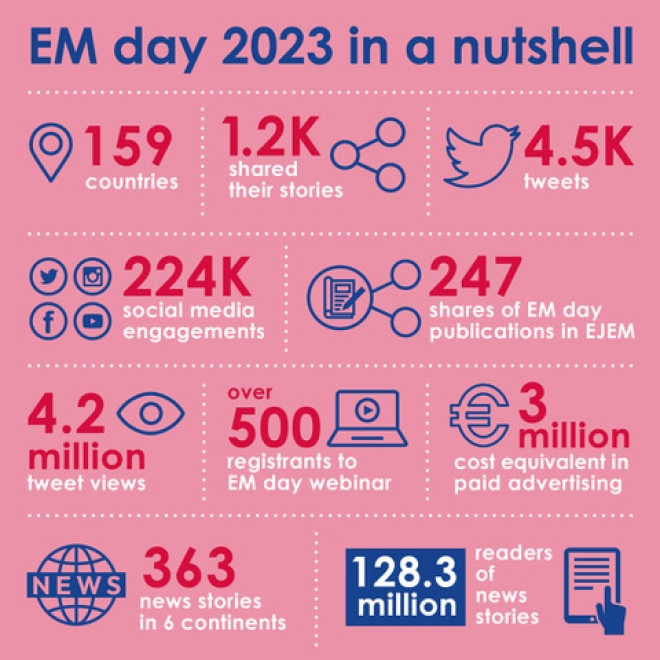
We would like to take this opportunity to thank everyone who took part in this year’s campaign. As you can see from the infographic, we had a global outreach of over 120 Million people across 6 continents, coming from 159 countries.
A big thank you to the national societies, international organisations and patient organisations for their support for this campaign, as well as to the individual EM doctors, nurses, paramedics and the general public who helped to create great awareness of patient safety in the ED. There were many activities taking place on May 27, from symposia to festivals to fun runs!
The results of an international survey, published in the European Journal of Emergency Medicine to coincide with EM Day, found that professionals felt that neither themselves nor their patients were safe enough in Emergency Departments. The staff felt under-supported by their hospital managements and did not have the right tools to provide adequate care. They also felt they were under too much pressure to meet external targets at a time when the whole EM system is under strain. We once again highlighted the issue of an overworked workforce trying to manage patients in failing healthcare systems that do not tackle the problem of patient safety but instead add unnecessary risk.
We will be publishing a paper analysing the results by country in the near future. We hope that societies will use this information to continue the campaign at national level.
There needs to be a recognition that Emergency Medicine is not simply the gateway to other departments. It is well known that patients who are treated quickly have a better outcome. Overcrowding needs to be addressed by better coordination and communication between different departments. Patients deserve a healthy workforce that is neither overtired, nor mentally drained.
We advocate for healthcare systems, governments, the general public and policymakers to support our emergency medical services and make the changes necessary to create an environment where patients and EM healthcare professionals feel safe.
We look forward to next year’s campaign where we hope to have an even larger engagement and a bigger impact! Thank you once again, and see you next year!
Dr Roberta Petrino
EM Day Working Group Chair
Dr Luis Castrillo
EM Day Working Group Co-Chair